Hello,
I am Samantha Workman. I am a graduate student at Western Illinois University. I conduct research here at Western with Dr. Afitlhile. Our main focus is on lipid biochemistry but more generally molecular biology. I enjoyed my time here as an undergrad sooo much that I decided to jump right into a masters program after graduating! Its been a lot of work but will be worthwhile. I only wish I would have had some mycology classes in my undergrad because fungi are super cool and interesting. Hope you enjoy my blog on Wangiella!
I am Samantha Workman. I am a graduate student at Western Illinois University. I conduct research here at Western with Dr. Afitlhile. Our main focus is on lipid biochemistry but more generally molecular biology. I enjoyed my time here as an undergrad sooo much that I decided to jump right into a masters program after graduating! Its been a lot of work but will be worthwhile. I only wish I would have had some mycology classes in my undergrad because fungi are super cool and interesting. Hope you enjoy my blog on Wangiella!
Taxonomic
classification
Kingdom: Fungi
Phylum: Ascomycota
Order: Chaetothyriales
Genus: Wangiella
http://www.doctorfungus.org/thefungi/wangiella.php
Introduction to Wangiella
Distribution
Wangiella has a world-wide distribution and has been isolated from environmental samples such as soil, plant materials, and mulch beneath pine trees in the United States (6). It is especially prominent in the tropical and subtropical regions of the world (5). This fungus was originally isolated by Dr. Kaiichiro Kano in Japan in 1933 and was described in 1934 (5). It is a dematiaceous (darkly-pigmented) fungi. It is a saprobic (decays organic matter) fungi as well (1).
Features
Being a pigmented fungus, Wangiella is characterized by having melanin in the cell walls of their saprophytic and parasitic forms (5). Colonies of Wangiella tend to grow very slowly, appearing after about 3 to 4 weeks of growth (1). It is quite often grown on potato dextrose agar (PDA) and does best at a temperature of 25 degrees C (1). The fungus appears yeast-like, moist and shiny. The color of growth will be black.

Colonies of Wangiella photo courtesy of www.Dr.Fungus.org


Wangiella conidiophore form (left) and yeast form (above).
Photos courtesy of www.DrFungus.org
Pathogenicity and Infection in Humans
Wangiella can be an agent in causing subcutaneous phaeohyphomycosis (2). Phaeohyphomycosis is a superficial or deep infection of the skin and other areas that is most often caused by a fungus dark in color (2). The infection can be caused by traumatic implantation of the fungus through the skin. This is a neurotropic fungus, which means it has an affinity for localizing selectively in nerve tissue. There have been cases of Wangiella infecting the central nervous system. It has also been shown to cause keratitis, pneumonia, and endocarditis (1). In patients with compromised immune systems, Wangiella can cause disseminated infections.
Subcutaneous Phaeohyphomycosis infection by Wangiella

(Image Courtesy of www.doctorfungus.org @ 2005)
Clinical Cases
of Wangiella infections
Link: http://cid.oxfordjournals.org/content/23/1/197.full.pdf
Clinical case 1: A 70-year-old man who was immunocompetent was admitted to the Aga Khan Hospital (Pakistan) because of complaints of progressive weakness on the left side of his body (4). The patient was also drowsy with signs of left hemiplegia. The laboratory investigations showed leukocytosis. A CT scan of the head showed a ring-enhancing lesion in the right lobe of the brain, which was initially diagnosed as brain abscess (4). A crainotomy was performed in which a thick, brown pus was recovered. A gram stain did not reveal any bacteria, however a fungal smear showed a moderate number of septate hyphae (4). Amphotericin B was given as treatment. The patient's condition improved greatly after the first week of treatment. However, on the 12th day the family took him home against medical advice and the patient died two weeks later (4). The initial pus was inoculated on Sabouraud dextrose agar and was confirmed to be Wangiella dermatitidis.
Link: http://cid.oxfordjournals.org/content/23/1/197.full.pdf
Clinical case 1: A 70-year-old man who was immunocompetent was admitted to the Aga Khan Hospital (Pakistan) because of complaints of progressive weakness on the left side of his body (4). The patient was also drowsy with signs of left hemiplegia. The laboratory investigations showed leukocytosis. A CT scan of the head showed a ring-enhancing lesion in the right lobe of the brain, which was initially diagnosed as brain abscess (4). A crainotomy was performed in which a thick, brown pus was recovered. A gram stain did not reveal any bacteria, however a fungal smear showed a moderate number of septate hyphae (4). Amphotericin B was given as treatment. The patient's condition improved greatly after the first week of treatment. However, on the 12th day the family took him home against medical advice and the patient died two weeks later (4). The initial pus was inoculated on Sabouraud dextrose agar and was confirmed to be Wangiella dermatitidis.
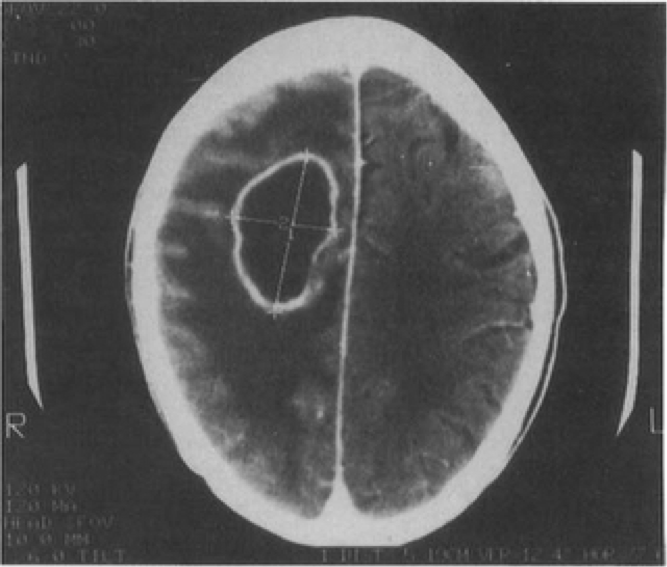
Contrast-enhanced
CT scan of the brain of a patient with an abscess due to Wangiella dermatitidis
showing a ring-enhancing lesion with cerebral edmea.
http://cid.oxfordjournals.org/
Note: Central nervous system cases of phaeohyphomycosis due to Wangiella dermatitidis are extremely rare, and most documented cases have not occured outside of Asia (7). Only six documented cases of Wangiella dermatitidis as a causative agent of brain infections have been reported in the world (7).
http://cid.oxfordjournals.org/
Note: Central nervous system cases of phaeohyphomycosis due to Wangiella dermatitidis are extremely rare, and most documented cases have not occured outside of Asia (7). Only six documented cases of Wangiella dermatitidis as a causative agent of brain infections have been reported in the world (7).
Clinical cases
of Wangiella infections
Link: http://jcm.asm.org/content/34/4/1011.short
Clinical case 2: A 3-year-old male with stage C-3 vertically acquired HIV type 1 infection was admitted to the hospital for a fever and a positive blood culture (3). He had previously been hospitalized many times for opportunisitc infections. Therefore he was receiving a continous zidovudine infusion through a central venous catheter (3). Three days before his admission, he was treated as an outpatient for a new fever of 38.9 degrees C. Blood cultures were drawn from the central venous catheter and from a peripheral vein, and vancomycin therapy was started (3). However, three days later yeastlike fungi were found in one of the catheter blood cultures, and further evaluation was done. After further evaluation, vancomycin treatment was discontinued and amphotericin B treatment was started (3). Three days later, yeastlike fungi was again recovered from the catheter and all isolates were later identified as Wangiella dermatitidis. The diagnosis was catheter-associated fungemia, and the catheter was removed. The patient was discharged and amphotericin B treatment was continued. However, three weeks later a new catheter was inserted and the patient developed swelling, tenderness, and erythema at the catheter site (3). Amphotericin B was restarted and after a month was changed to itraconazole. No further fungal infections were detected.
Link: http://jcm.asm.org/content/34/4/1011.short
Clinical case 2: A 3-year-old male with stage C-3 vertically acquired HIV type 1 infection was admitted to the hospital for a fever and a positive blood culture (3). He had previously been hospitalized many times for opportunisitc infections. Therefore he was receiving a continous zidovudine infusion through a central venous catheter (3). Three days before his admission, he was treated as an outpatient for a new fever of 38.9 degrees C. Blood cultures were drawn from the central venous catheter and from a peripheral vein, and vancomycin therapy was started (3). However, three days later yeastlike fungi were found in one of the catheter blood cultures, and further evaluation was done. After further evaluation, vancomycin treatment was discontinued and amphotericin B treatment was started (3). Three days later, yeastlike fungi was again recovered from the catheter and all isolates were later identified as Wangiella dermatitidis. The diagnosis was catheter-associated fungemia, and the catheter was removed. The patient was discharged and amphotericin B treatment was continued. However, three weeks later a new catheter was inserted and the patient developed swelling, tenderness, and erythema at the catheter site (3). Amphotericin B was restarted and after a month was changed to itraconazole. No further fungal infections were detected.

Slide culture showing
oval conidia and tapered conidiophores of W. dermititidis. The stain used
was lactophenol cotton blue. photo courtesy of Nachman et al (1996)
Websites with more info on Wangiella:
www.doctorfungus.org/thefungi/wangiella.php
www.sbs.utexas.edu/mycology/wangiella_dermatitidis.htm
www.mold.ph/wangiella-dermatitidis.htm
www.doctorfungus.org/thefungi/wangiella.php
www.sbs.utexas.edu/mycology/wangiella_dermatitidis.htm
www.mold.ph/wangiella-dermatitidis.htm
References
1. http://www.doctorfungus.org
2. http://www.mold.ph/wangiella-dermatitidis.htm
1. http://www.doctorfungus.org
2. http://www.mold.ph/wangiella-dermatitidis.htm
3.
Nachman, S., Alpan, O., Malowitz, R., and Spitzer, E. 1996.
Catheter-Associated Fungemia Due to Wangiella (Exophiala) dermatitidis.
Journal of Clinical Microbiology 34: 1011-1013.
4. Ajanee, N., Alam, M., Holmberg, K., and Khan, J. 1996. Brain Abscess Caused by Wangiella dermatitidis: Case Report. Clinical Infectious Diseases 23: 197-8.
5. Matsumoto, T. 2000. Wangiella Dermatitidis Infections: A Paradigm of the Opportunistic Mycoses Caused by Black Yeasts and Moulds. Kor J Med Mycol 5: 45-50.
4. Ajanee, N., Alam, M., Holmberg, K., and Khan, J. 1996. Brain Abscess Caused by Wangiella dermatitidis: Case Report. Clinical Infectious Diseases 23: 197-8.
5. Matsumoto, T. 2000. Wangiella Dermatitidis Infections: A Paradigm of the Opportunistic Mycoses Caused by Black Yeasts and Moulds. Kor J Med Mycol 5: 45-50.
6. Lye, W.C. 2011. Peritonitis Due to Wangiella Dermatitidis in a Patient on CAPD. Peritoneal Dialysis International 1.
7. Chang, C., Kim, D., Park, D., Kim, H., Lee, C., and Shin, J. 2000. Acute Cerebral Phaeohyphomycosis due to Wangiella dermatitidis Accompanied by Cerebrospinal Fluid Eosinophilia. Journal of Clinical Microbiology 38: 1965-66.